
Equipment, Supplies, Instruments
Dental Operating Units contain high-speed handpieces, suction, and an air-water syringe. For short-term missions, they must be transportable as a carry-on bag or as an airline, 50-pound or less, checked bag. Reliable examples include:
Aseptico’s, 34-pound, self-contained Task Force Deluxe unit works on 110-240 Volts and uses a standard four-hole connection for handpieces. The CDS rents this unit for missions. If not carried as a checked bag, it needs to be protected when shipped as an airline-checked bag.
Aseptico’s, 34-pound, self-contained GO unit works on 110-240 Volts and uses a electric handpiece with interchangeable heads. The unit can be purchased from Aseptico and they give a 20% discount if used for missionary endeavors.
The CDS also has a battery-operated dental unit which can be rented and, if interested, contact the CDS.
Aseptico’s, lightweight portable, compressed air units require compressed air to operate and are an option, especially if compressed air is available; the CDS rents these units.
The CDS rents a portable compressor that works with the compressed air unit.
Med Missions: www.medmissions.org/dental rents portable dental units and equipment.
When you do not have electricity and need a handpiece for surgery (to section a tooth or remove bone) or doing limited restorative (cutting or smoothing), a battery-operated handpiece can be used. For suction, a DeVilbiss Portable Suction Unit 7305DD like the one shown in the hygiene kit may be used and can be purchased with a battery. The angled, small-tipped, white disposable suction tips for surgery and the angled, medium-sized tipped, green disposable suction tips for restorative are suggested. Field substitutes for air and water syringes are two 30-50 cc syringes with disposable tips.
Equipment items to perform dentistry comfortably where there is not a clinic include a lightweight, durable, easily transportable, patient chair and operator stool that provides back support. CDS loans and recommends the 13-pound, corrugated plastic chair that will hold a 450-pound patient and the two-pound, Camp-Time, dental stool found under the Equipment section.
To take X-rays, the CDS rents a Nomad, portable x-ray unit, but a personal computer and scanner must be brought by the clinician. As an alternative, Google and purchase Dentafilm, Ergonom-X self-contained film with fixer and developer. The majority of smaller, short-term trips do not take X-rays.
Sterilize instruments to avoid the spread of disease (do not settle for cold disinfection). The CDS recommends the Presto, four-quart, stainless steel pressure pot which can be heated with whatever is used to heat water, is certified as a field sterilizer, and has a total cycle of only 20 minutes. Look under “Equipment and Kit Rentals” under “Field Sterilization in 10 Minutes” for instructions, a letter of certification, and an instructional video.
Other equipment items include a curing light per provider ($25-30), handpieces ($20-30), a composite gun per provider ($6-8), and a blood pressure set-up that can be purchased inexpensively on E-bay or Amazon.
Hygienists should travel with an ultrasonic and suction. See the CDS Hygiene Kit under “Equipment and Kits” then “Rentals under Hygiene Kit.” On the mission field, it is usually not time effective to do polishing as the needs are so great.
Amalgamators are being used less and less. Amalgam and some Glass-Ionomers require titration. Glass-Ionomers are now available in mixable paste options and amalgam is rarely used anymore, but amalgam is still an excellent restorative material. If using an amalgamator in the Eastern hemisphere, make sure it works on 220-240 Volts or take a transformer that will accommodate the motor.
Loops and a headlight are essential and standard in the U.S., but not in the developing world. Suggest carrying your expensive, fragile loops and headlight in your backpack or carry-on bag. An inexpensive ($16), re-rechargeable, lightweight, reliable, adjustable headlight is the GOfORWild brand found on Amazon.
Transformers to change from 110-120 Volts to 220-240 Volts is rarely required now. Almost everything works on 110-240 now and can be confirmed by checking voltage information found on the unit or plug-in. Computers, cell phones, curing lights, headlights, hairdryers, curling wands, coffee pots, newer amalgamators, etc. all work everywhere.
Dental supplies are costly and expire. Many are disposable, can be operator-specific, and are needed in the right amounts, thus calculating dental supplies for any trip presents challenges.
Acquire as much information as possible ahead of time to figure out the total hours of actual patient treatment time (each day’s hours of treatment time can vary greatly), type of treatment (surgery vs. restorative), number of operators, experience of the operators (students vs. experienced), as well as the availability and competence of interpreters and assistants all need to be considered. Suggest planning for 20% over and bring home or donate locally what you do not use.
Check in advance about supplies available in the international country. Generally, dental teams like to take all the supplies they need in checked bags so they are ready to go and know exactly what they have.
Check expiration dates on all supplies as customs may confiscate outdated materials. They do not usually check items like gloves, needles, burs, and disposables (which all have expiration dates), but are more concerned about medications, anesthesia, and restorative supplies.
A chart example to calculate disposable supplies is listed on page 71 of the Dental Mission Manual for Portable, Short-Term Dental Trips.
There are numerous avenues to acquire dental supplies including:
- Supplying from your office if you cannot get them donated.
- Talk to other dental offices and ask for contributions.
- Talk to your dental supply representative (Henry Schein, Patterson, Benco, Burkhart, and others.
- Talk and request supplies from dental companies such as Septodont, GC America, Ultradent,
- Brasseler, glove companies, Henry Schein Cares, and others.
- Talk to your Sunday School class, church, friends, neighbors, and family, and consider writing a letter of support with several examples on pages 210-214 of the Dental Mission Manual.
- These personal connections often donate toothbrushes and finances to help worthy causes.
- World Dental Relief: www.dentalrelief.com for dental supplies.
- Blessings International: www.blessings.org/blog-post/dental-supplies
- Map International has medical supplies; www.map.org
- Purchase supplies inexpensively from internet sites like E-bay and Amazon.
- Hygienists can obtain supplies, instruments, and equipment from the CDS Hygiene Kit.
Restorative supplies and an anesthesia kit for each dentist can easily be stored in plastic, fishing tackle boxes purchased where fishing supplies are sold.
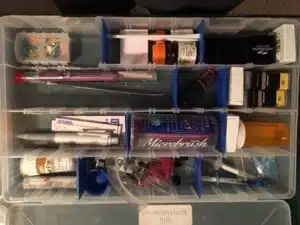
Two Examples of a Restorative Kit Holding Dental Supplies Includes a Bur Block.

A dental anesthesia kit holds a composite gun, bib clip, floss, and items needed chairside for anesthesia in a small plastic container.
Calculating which instruments and how many to take on a mission trip requires knowing the number of providers, the type of treatment planned (% of restorative, surgery, and hygiene), sterilization turn-around time (with the Presto pressure pot, the instruments are back in about 20 minutes), and the experience level of the dental team members.
Recommend not bagging (as reusing and not storing or making packs of instruments). Just get the instrument needed for the procedure from a common area. Consider getting plastic trays to hold and transport patient instruments and cover them with half a bib, using the other half for the patient.
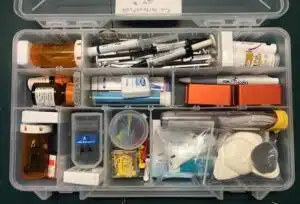
Recommend storing and transporting instruments in plastic, fishing tackle boxes. See Examples:


For Surgery, Plastic Containers for Forceps and Elevators/Luxators for Numerous Dentists

A Plastic Container for All Other Surgical Instruments, Sutures, and Blades


Plastic Containers for Rubber Dam Set-ups and Restorative Instruments for Several Dentists
There is a Garrison Interproximal Set-up and #12 blades with Bard-Parker Handle (Center/Right)
Scalers and Curettes on the Left, Second from the Bottom
Generally, if treating a combination of restorative and surgery patients, three sets of instruments are recommended per provider. If doing primarily surgery, four or even five set-ups of surgical instruments are suggested, as surgical procedures are generally faster than restorative. Plan on having an anesthetic syringe for each kit and a few extra mirrors and explorers for exams and consultations. Take a few periodontal probes, scalers, and curettes.
Recommend the sterilization station prepare an exam kit for each patient by placing an anesthetic syringe, mirror, and explorer on a plastic tray with a half bib which becomes the dirty tray for transporting and holding instruments and supplies. Suggest storing the syringes, mirrors, explorers, and bib clips at sterilization in a single plastic container.
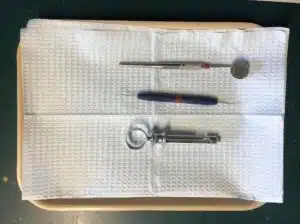

Exam Tray Prepared Ahead for Each Patient Storage: Syringes, Mirrors, Explorers, & Bib Clips
Instruments can be obtained from numerous resources:
- Take instruments from your office.
- Rent instrument kits from the CDS by going to the “Equipment and Kits Rentals” section.
- World Dental Relief rents surgical instrument kits at www.dentalrelief.org.
- Consider Googling Amazon or E-bay to purchase inexpensive instruments.
- Ask for donations and missionary discounts from dental instrument suppliers
Some surgical instrument considerations include:
- Forceps with serrated beaks grip the tooth better, especially for rotational movements.
- Upper and lower universal forceps (pedo and regular) remove most teeth.
- Consider a #23 Cowhorn for lower molars and a #88R and L for upper molars.
- Carry one each upper and lower needle forcep.
- Try the Woodson #1 for tissue reflection; they work great, and do not crush the tissue.
- Luxators get out roots and are often more useful than elevators.
- Vicryl sutures resorb by hydrolysis, not inflammation like gut, are easy to tie, and can be used sub-durally as a universal suture without having to worry about removing them. Use Vicryl 4-0 on a FS-2 needle for most cases and for fine suturing use a 5-0 on a P-3 needle.
- 15c blades are smaller and easier to use than a 15-blade.
- Use bite blocks for lower extractions to protect the TMJ.
When hoping to restore a tooth, but questioning a tooth’s restorability or the nerve’s condition, inform the patient, “I want to save the tooth, but there is a lot of decay. I will numb the tooth and see if I can remove the decay and repair the tooth. If not, I will extract the tooth. Is that OK?” The patient generally expects an extraction. If you save the tooth, you are a hero and have not disappointed the patient if you have to extract.
On the mission field where there are more needs than you can fulfill, do the greatest good for the greatest number, concentrating on one area of the mouth based on what is best for the patient.
Two examples: 1. Choose to fix front teeth rather than extracting hopeless, posterior teeth. 2. Concentrate on fixing permanent teeth before addressing primary teeth unless primary teeth are really hurting, infected, or interfering with the eruption of the permanent teeth. If possible, patients can come back for a second round of treatment.
Controlling the “Gate” or access to care and setting up reasonable expectations is very important, as the dental team can never hope to meet all of the dental needs. In most situations, the dental team leader is responsible for determining the number of patients that can reasonably be treated each day (save room to treat the pastor and helpers, as almost everyone needs dental care). The team leader evaluates treatment capabilities in surgery, restorative, hygiene, specialty, and preventive care. The team focuses on treating the patient’s chief complaint. This information is carefully and tactfully communicated to the local leader or representative, who best understands and discerns local population dynamics to balance patient’s expectations with the team’s capabilities. The responsibility of controlling access to dental care is given to the locals who are encouraged to make a list or hand out numbered cards to patients to be seen. Ideally, if done successfully, at the end of the day, expectations are met, all feel blessed, and no one is upset. It is more important to leave a Godly, loving impression than to count procedures.
